.png)
As an evidence-driven organisation, we aim to base all our key decisions on data. To achieve this, we needed to conduct research before launching our pilot campaign in Kano State. In particular, we needed to ensure that we had a proper understanding of the local context.
Our key questions were:
Who is our target audience? (what do they value, how do they live, and who are their role models.)
What factors encourage or discourage contraceptive use in Kano?
How should we structure our content?
To answer these questions, we took a cluster approach: drawing on multiple different research tools and combining the results to build a better picture of the landscape. Some of the methods we used included literature reviews, surveys, interviews, and focus group discussions. (For more information about the tools we used, and their strengths and weaknesses, see the appendix.)
Overall, we spent more than 190 hours on desk research, and interviewed more than 300 radio listeners. Our findings, outlined below, ultimately resulted in our pilot campaign, which launched on World Contraceptive Day, in collaboration with the Ministry of Health. The campaign is currently on air in Kano State, Nigeria, and is now reaching 5.6 million listeners through our partner station.

Picture 1: The leftmost photo is from our expert workshop and the rightmost is of three of the surveyors on our team.
1. Who is our target audience?
Our pilot campaign in Kano State was primarily aimed at married couples with children. There were three main reasons for this. First, due to cultural concerns, our Nigerian stakeholders were not comfortable with us targeting unmarried women. Second, relevant studies demonstrated larger effect sizes within these groups. Third, experts had advised that our messaging was unlikely to impact newlywed couples, as the pressure to have a child soon after marriage is very strong. Given these factors, it seemed most impactful to focus on couples who already had children, and who wanted to space or limit future births.
However, to create content that resonated with this audience, we needed to know more about them. What was most important to them— what were their values and dreams? What were their daily routines and joys? Who were their role models?
To investigate, we drew on a mix of qualitative research (one-to-one interviews and focus group discussions with listeners,) expert opinion, barrier analysis surveys, and interviews with clinic workers. (See the appendix for further information about these research tools). Our findings suggested that:
Family, education, and economic success were important values Providing proper care to their children and others in the community was an important value for both men and women. Both men and women also cited the importance of peace and harmony. They wanted their children to become contributing members of the community and to have “good values.” Some women wished for more education for themselves, and men wanted to improve their business and earning prospects.
Work dominated daily routines, while religion and the radio were common sources of joy Womens’ daily routines often consisted of preparing children for school, praying, housework, and cooking while listening to the radio. Some sold spices or other things from home. Men cited work as important to their daily routine, and spent considerably less time on childcare and household chores. Generally, men seemed to be responsible for financial provision and women for housework and childcare. Women told us that listening to the radio while doing chores was the highlight of their days, while men cited religious activities instead.
Family and religious figures were important role models For women, important role models included mothers and other senior family members such as aunts and older sisters. Female neighbours were also mentioned as significant. Men, on the other hand, listed only their fathers and the prophet Muhammad as their role models.
Developing personas
After analysing these findings, we developed six personas— imaginary characters meant to exemplify the typical target listener— to guide and inspire our in-country content writers. You can see our personas here.

Picture 2: Personas created to inspire our writers to produce material that our target audience can relate to.
2. What factors encourage or discourage contraceptive use in Kano?
To create impactful radio messaging, we needed to know which factors have the greatest influence on contraceptive use or non-use in our local context. To investigate, we conducted several surveys, interviews, and focus group discussions, as well as a literature review. (For further details, see the appendix outlining our research tools).
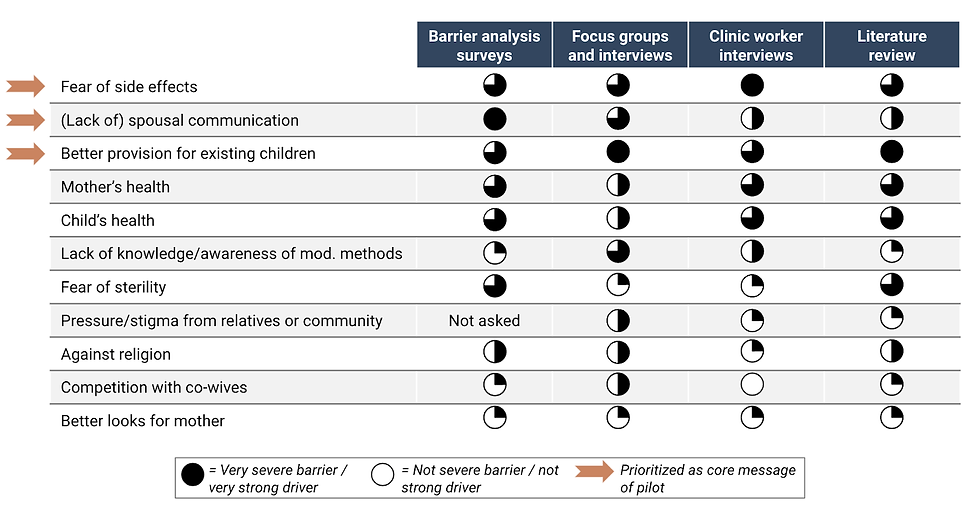
Picture 3: Results of our research from 4 select tools. The barrier analysis survey and focus groups and interviews were conducted with target listeners.
Combining the results of these various lines of research revealed three key findings:
Fear of side effects is a significant barrier to contraceptive use Both women and men had numerous concerns about side effects. Those mentioned most often included fear of sterility, irregular or heavy menstrual cycles, and contraceptive implants or IUDs moving within the body after being inserted. Despite these concerns, research participants generally recognised the value of seeking advice from health professionals, and were aware that there were unhelpful rumours about side effects.
Lack of spousal communication is also a common obstacle Many of the people we surveyed found it difficult to discuss family planning with their spouse/s. Women often feared that raising the subject would anger or upset their husbands, and some men had similar concerns. We also heard conflicting views as to who should be responsible for family planning decisions. Women typically felt that this was the husband’s role, while men’s views were more variable. Our research also suggested that spouses discussing family planning can lead to a greater fear of side effects. Therefore, it seemed important to address both factors together.
Care for existing children is a strong motivator for family planning Many research participants saw family planning as enabling better care for existing children. For example, one said that “childbirth spacing... can provide you more time to take care of the children properly”. Many participants also noted the importance of having more money, per child, to pay for education, food, and clothing. Providing sufficient time and money was often seen as necessary to raise “children that you’ll be proud of”.
Although these three factors were the most important, they did not outrank other influences on contraceptive use by a particularly large margin. (I.e. they did not follow a power law or Pareto distribution). As can be seen in the graph below, several barriers and drivers had a similar level of impact/importance.

Picture 4: Relative importance of barriers and drivers in Kano State, Nigeria. Based on a weighted average of scores derived from various research tools.
Given these findings, it seemed most impactful to address many different barriers and drivers. Consequently, our pilot campaign covers the top 11 barriers and drivers above, with a greater emphasis on the top three.
3. How should we structure our content?
Targeting the right barriers and drivers wasn’t the only factor to consider. We also wanted to investigate the role of other variables, such as the length and frequency of our broadcasts. Again, we drew on a range of tools, including expert opinion, a literature review, a landscape analysis, and empirical prototyping tools. (See the appendix for further information about our research tools).
Our findings suggested that:
Ads and shows should air frequently, with some repetition Drawing on the results of other social behaviour change (SBC) campaigns, we concluded that our long-form shows should air once or twice per week. It also seemed beneficial to air reruns, with each episode of the show being broadcast up to 3 times, and each ad airing at least 70 times.
Shows should be on the longer side and incorporate storytelling or Q&A Our review of other SBC campaigns suggested that longer shows tend to be more impactful. Several different show types have been successful, but there was the most support for drama, storytelling, and call-in/Q&A style shows.
Content should be positive, gentle, and specific Based on evidence from the fields of psychology and marketing, a positive, gentle and informal/peer-to-peer tone seemed likely to be the most persuasive. We also concluded that specific messaging would be more impactful than more general statements.
Our next steps
We completed this research in June, and are currently broadcasting our pilot on Freedom Radio in Kano. Our pilot has two parts and will last six months. Prior to launch, we conducted a 950 person baseline survey. After three months of the campaign, we’ll conduct a midline survey, and after a further three months we’ll conduct the endline survey. By August next year, we should know whether or not we were able to change attitudes, knowledge, and behaviour around contraceptive uptake. If the results are positive, we plan to scale rapidly while potentially conducting a more rigorous randomized evaluation.
How you can help
Donate We have room for more funding, and Giving Tuesday is an especially good time to donate. For $1,620, you can sponsor a week’s worth of advertisements and shows (airtime) reaching 5.6 million listeners.
Provide technical advice We’re interested in speaking with more academics and other experts on family planning, social and behavior change interventions, and qualitative research.
Volunteer for short- or long-term engagement We’ve identified numerous opportunities for volunteers to support us from anywhere in the world. You can express interest in opportunities here and read more about them here.
We look forward to hearing from you! Please feel free to reach out to us directly with your feedback, questions, or ideas.
Appendix: How we approached our research
Every research tool has its limitations. Given that, we believe applying a cluster approach is the best way of coming to reliable answers. Cluster thinking involves investigating an issue from multiple different perspectives and looking for areas of agreement. If many different models point in the same direction, we can be more certain of the results.
Some of the research and prototyping tools we drew on included:
Expert opinion: We invited 40 health experts, government workers, religious leaders, and radio experts from Kano State, Nigeria, to participate in a discussion workshop. Together, these experts shared their views on which barriers to contraceptive use were most prevalent. As well as offering a great deal of qualitative feedback, participants ranked each barrier according to its addressability and importance.
Behaviour change theories: There are many theories about what influences people to adopt different behaviours. We reviewed some of the relevant literature and applied the best-supported theories to our research questions.
Landscape analysis: We examined what other organisations in the social and behavioural change (SBC) space currently do, and what they consider best practice.
Literature reviews: We completed two large literature review projects: one on factors influencing contraceptive use and non-use in northern Nigeria, and another exploring the features of the campaign. In total, 300 abstracts were scanned for relevant data. Although these reviews helped us understand the overall landscape well, the evidence base was not very strong.
Focus group discussions: We conducted 8 focus group discussions, each with five participants. These discussions focused on understanding our target audience’s interest, needs, and values. While this tool is great for showing which answers are considered socially or culturally appropriate, it may be subject to social desirability bias. (I.e. participants may feel pressured to give socially acceptable answers instead of honest ones).
In-depth interviews: We conducted 8 in-depth interviews, also aimed at understanding our target audience. The one-on-one nature of this method helps reduce some, though not all, social desirability bias. However, conducting enough interviews to ensure that the answers are representative would be costly.
Barrier Analysis survey: We interviewed 45 women who were currently using modern contraceptives and 45 who were not, aiming to understand the differences in their attitudes and knowledge. Using that data, we were able to analyse the prevalence of different attitudes and how they differed between users and nonusers, indicating their possible effects on behaviour.
Clinic visit interviews: We interviewed 29 health workers from randomly selected clinics across Kano State. Their feedback helped us learn more about typical contraception users and the questions women and men have when they visit clinics.
Head-to-Head comparisons: We conducted 450 head- to head comparisons of 20 prototype ads, to better understand which features were effective. In each comparison, we showed participants two ads and asked them which they liked best across 5 criteria.
Qualitative feedback on material: We conducted 4 focus group discussions seeking qualitative feedback on the strengths and weaknesses of our ads.
Voice-over: 15 radio listeners listened to our programs and recorded their thoughts without any surveyors present. To achieve this, we developed a simple visual interface which participants could use to play a recording of our questions, and of the ads we wanted feedback on. Sharing feedback completely anonymously should help reduce social desirability bias. However, many participants found the interface difficult to use.
Survey We completed a baseline survey of 950 female radio listeners who are not looking to have a child within the next six months.
Comments